Download 680 Form in PDF
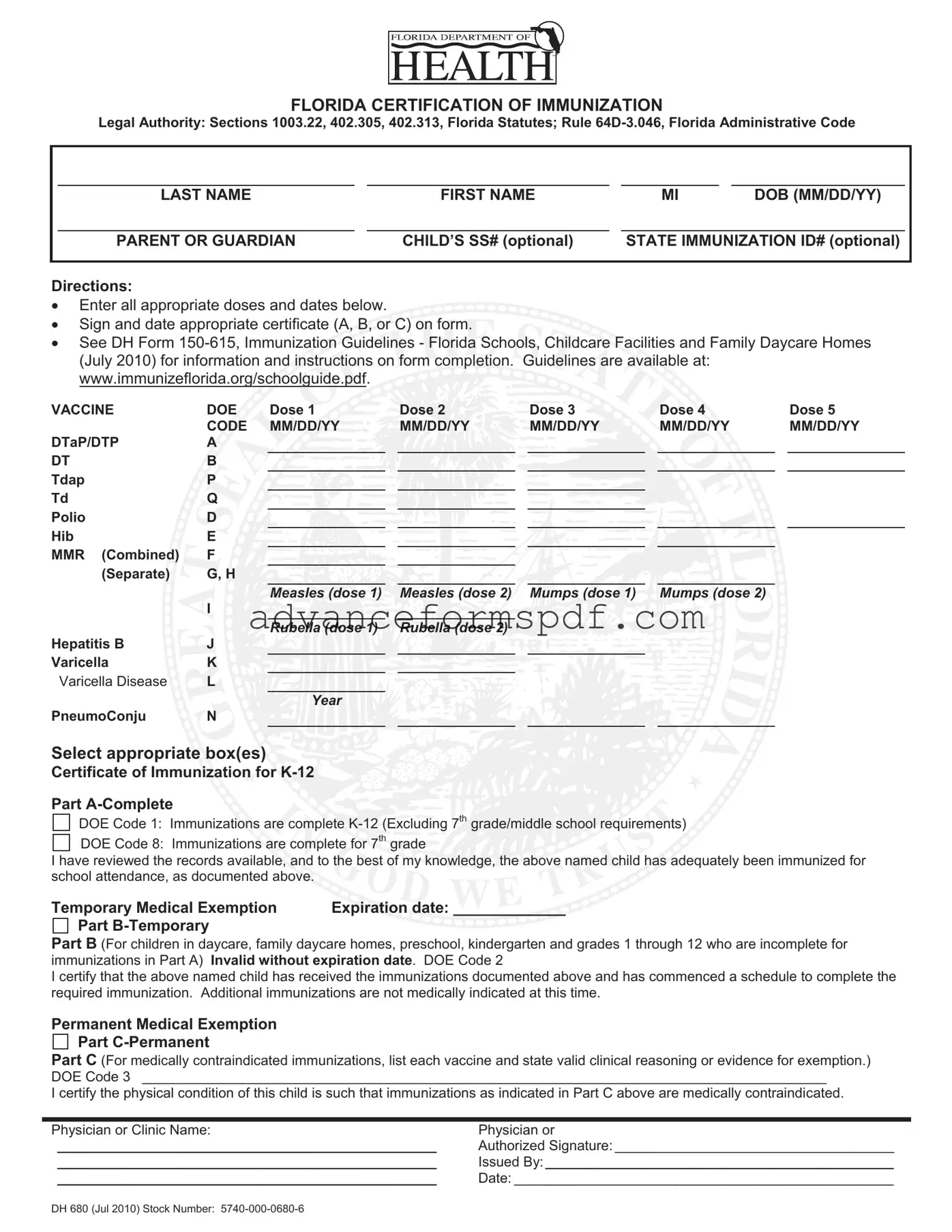
The Florida Certification of Immunization, commonly referred to as the 680 form, plays a crucial role in ensuring that children meet the vaccination requirements for school attendance in Florida. This form is governed by several legal authorities, including specific sections of the Florida Statutes and the Florida Administrative Code. It serves as a comprehensive record of a child's immunization history, detailing various vaccines administered, along with their respective dates. Parents or guardians are responsible for filling out the form, which includes sections for the child's name, date of birth, and optional identification numbers. The 680 form consists of multiple parts, allowing for different certification statuses: complete immunization records, temporary medical exemptions, and permanent medical exemptions. Each section requires careful documentation and must be signed by a qualified physician or clinic representative. Additionally, guidelines for completing the form are available through the Florida Department of Health, providing essential instructions for parents and guardians. This form not only facilitates compliance with state regulations but also promotes public health by ensuring that children are protected against preventable diseases.
Document Data
| Fact Name | Description |
|---|---|
| Legal Authority | The Florida Certification of Immunization is governed by Sections 1003.22, 402.305, and 402.313 of the Florida Statutes, along with Rule 64D-3.046 of the Florida Administrative Code. |
| Purpose | This form certifies that a child has received the necessary immunizations required for school attendance in Florida. |
| Immunization Records | Parents or guardians must enter all appropriate vaccine doses and dates on the form to ensure compliance with state requirements. |
| Certificate Types | The form includes three parts: Part A for complete immunizations, Part B for temporary exemptions, and Part C for permanent medical exemptions. |
| Guidelines Availability | Detailed immunization guidelines can be found at www.immunizeflorida.org/schoolguide.pdf, providing crucial information for form completion. |
| Expiration Dates | For temporary medical exemptions, an expiration date must be provided; otherwise, the exemption is invalid. |
How to Write 680
Filling out the Florida Certification of Immunization Form 680 is an essential step in ensuring your child meets school requirements. This form captures important immunization information and helps schools verify that students are up to date on their vaccinations. Here’s how to fill it out correctly:
- Gather necessary information: Collect your child's full name, date of birth, and the name of the parent or guardian. You may also need the child's Social Security number and state immunization ID number, though these are optional.
- Fill in personal details: Start with the last name, first name, middle initial, and date of birth in the designated fields.
- Complete the immunization section: For each vaccine listed, enter the date of each dose received in the corresponding fields. Make sure to provide all doses if applicable.
- Choose the appropriate certificate: Depending on your child's immunization status, check the box for either Part A, Part B, or Part C. Be sure to follow the guidelines for each part.
- Sign and date: The parent or guardian must sign the form, certifying the accuracy of the information provided. Include the date of signing as well.
- Review: Double-check all entries for accuracy. Ensure that all required fields are completed before submitting the form.
Once the form is completed and signed, it’s ready to be submitted to your child’s school or daycare facility. Keeping a copy for your records is also a good idea. This ensures you have proof of immunization should you need it in the future.
680 Example
FLORIDA CERTIFICATION OF IMMUNIZATION
Legal Authority: Sections 1003.22, 402.305, 402.313, Florida Statutes; Rule
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
FIRST NAME |
|
MI |
|
DOB (MM/DD/YY) |
|
|
|
|
|
|
|
|
|
|
|
PARENT OR GUARDIAN |
|
CHILD’S SS# (optional) |
|
STATE IMMUNIZATION ID# (optional) |
|
||
|
|
|
|
|
|
|
|
|
Directions:
Enter all appropriate doses and dates below.
Sign and date appropriate certificate (A, B, or C) on form.
or C) on form.
See DH Form 










VACCINE |
DOE |
Dose 1 |
|
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
CODE |
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
DTaP/DTP |
A |
|
|
|
|
|
|
|
|
|
DT |
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Tdap |
P |
|
|
|
|
|
|
|
|
|
Td |
Q |
|
|
|
|
|
|
|
|
|
Polio |
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Hib |
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MMR (Combined) |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
(Separate) |
G, H |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles (dose 1) |
|
Measles (dose 2) |
|
Mumps (dose 1) |
|
Mumps (dose 2) |
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rubella (dose 1) |
|
Rubella (dose 2) |
|
|
|
|
|
|
Hepatitis B |
J |
|
|
|
|
|
|
|
|
|
Varicella |
K |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Varicella Disease |
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year
PneumoConju N
Select appropriate box(es)
box(es)
Certificate of Immunization  K-12
K-12
Part
DOE Code 1: Immunizations are complete
DOE Code 8: Immunizations are complete for 7th grade
are complete for 7th grade
I have reviewed the records available, and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.
and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.


Temporary Medical Exemption |
Expiration date: _____________ |
Part |
|
Part B (For children in daycare, family daycare homes, preschool, kindergarten and grades 1 through 12 who are incomplete for immunizations in Part A) Invalid without expiration date. DOE Code 2
I certify that the above named child has received the immunizations documented above and has commenced a schedule to complete the required immunization. Additional immunizations are not medically indicated at this time.
Permanent Medical Exemption
Part
Part C (For medically contraindicated immunizations, list each vaccine and state valid clinical reasoning or evidence for exemption.) DOE Code 3 ________________________________________________________________________________________
I certify the physical condition of this child is such that immunizations as indicated in Part C above are medically contraindicated.
Physician or Clinic Name: |
Physician or |
_________________________________________________ |
Authorized Signature: ____________________________________ |
_________________________________________________ |
Issued By:_____________________________________________ |
_________________________________________________ |
Date: _________________________________________________ |
DH 680 (Jul 2010) Stock Number:
Common PDF Documents
Who Can Write an Esa Letter - This document confirms that an emotional support animal is essential for mental health support.
A Non-disclosure Agreement (NDA) is a legal contract that establishes a confidential relationship between parties, ensuring that sensitive information remains protected. In Arizona, this form is essential for businesses and individuals who wish to share proprietary information without the risk of it being disclosed to unauthorized entities. Understanding the nuances of the Arizona Non-disclosure Agreement can help safeguard your intellectual property and maintain your competitive edge. For further details, you can refer to Arizona PDF Forms.
Chick Fil a Job Application - Keen attention to detail for order accuracy.