Download Employee Accident Report Form in PDF
When an employee is involved in an accident at work, documenting the incident is crucial for both the employee and the employer. The Employee Accident Report form serves as a vital tool in this process. It captures essential details such as the date, time, and location of the accident, as well as a description of the events leading up to the incident. The form also includes sections for the names and contact information of witnesses, which can provide valuable insights into what happened. Additionally, it allows for the reporting of any injuries sustained, ensuring that the employee receives appropriate medical attention and support. By filling out this form, employees can help their employers understand the circumstances surrounding the accident, leading to better safety measures and policies in the workplace. Properly completed, this form not only aids in compliance with workplace safety regulations but also serves as a record for potential insurance claims or legal matters that may arise from the incident.
Document Data
| Fact Name | Description |
|---|---|
| Purpose | The Employee Accident Report form is used to document workplace accidents and injuries. It helps employers track incidents and ensures proper reporting for insurance and safety compliance. |
| Who Completes It | The form is typically completed by the employee involved in the accident or a supervisor who witnesses the event. Accurate information is crucial for effective follow-up. |
| State-Specific Laws | Each state may have specific laws governing the reporting of workplace accidents. For example, in California, employers must comply with Cal/OSHA regulations, which require detailed reporting of workplace injuries. |
| Importance of Timeliness | Filing the report promptly is essential. Many states have deadlines for reporting workplace injuries to ensure compliance with workers' compensation laws. |
How to Write Employee Accident Report
Completing the Employee Accident Report form is a crucial step in documenting any workplace incident. This report helps ensure that all relevant information is collected and can facilitate necessary follow-up actions. Follow these steps carefully to fill out the form accurately.
- Begin by entering your personal information, including your name, job title, and department.
- Provide the date and time of the accident. Be as precise as possible.
- Describe the location where the accident occurred. Include specific details to help identify the site.
- Detail the nature of the accident. Clearly explain what happened, including any equipment or materials involved.
- List any witnesses to the incident. Include their names and contact information if available.
- Indicate any injuries sustained. Be specific about the type and severity of the injuries.
- Sign and date the report to confirm that the information provided is accurate.
After completing the form, submit it to your supervisor or the designated safety officer. Timely submission is essential for ensuring that appropriate actions are taken following the incident.
Employee Accident Report Example
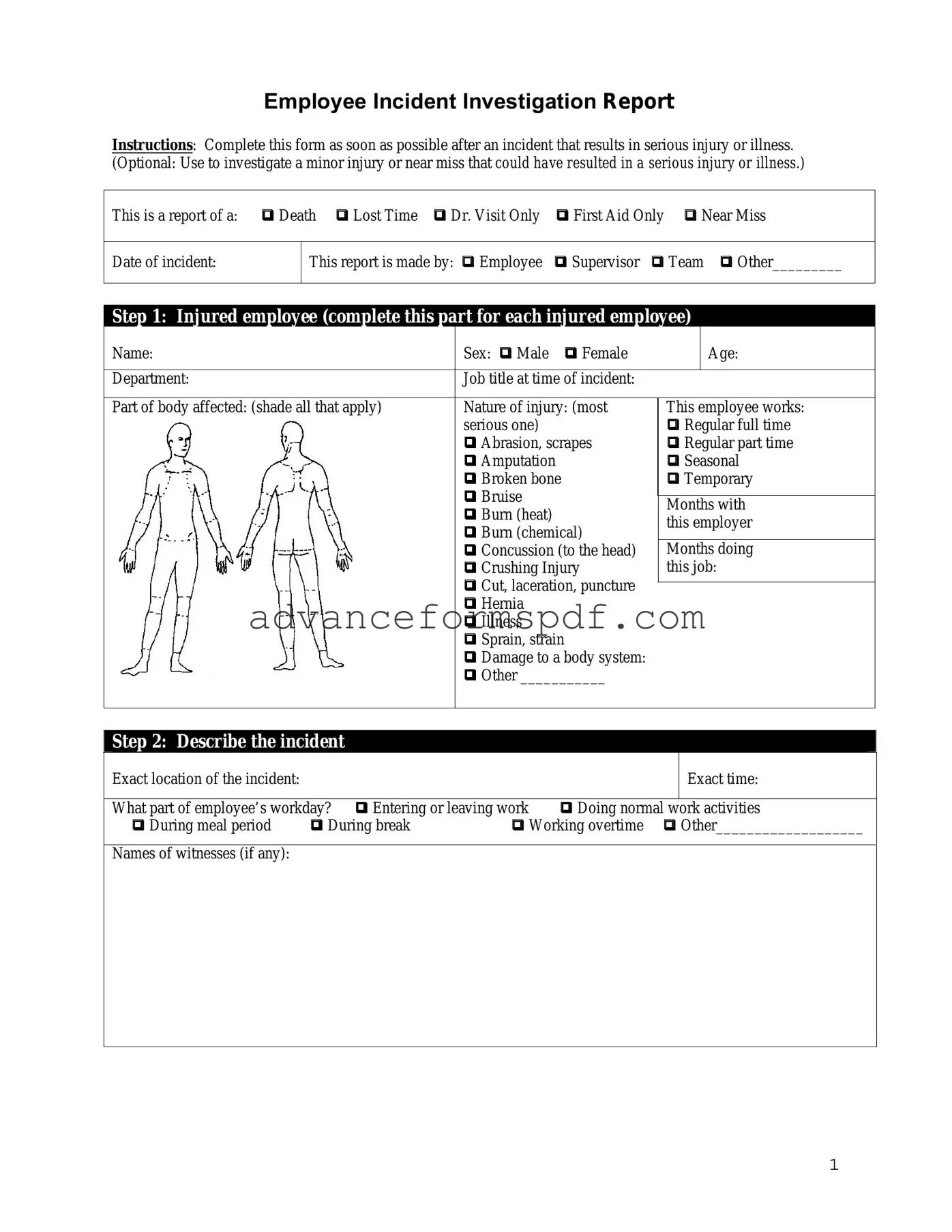
Employee Incident Investigation Report
Instructions: Complete this form as soon as possible after an incident that results in serious injury or illness.
(Optional: Use to investigate a minor injury or near miss that could have resulted in a serious injury or illness.)
This is a report of a: Death Lost Time Dr. Visit Only First Aid Only Near Miss
Date of incident:
This report is made by: Employee Supervisor Team Other_________
Step 1: Injured employee (complete this part for each injured employee)
Name: |
Sex: Male Female |
|
Age: |
|
|
|
|
Department: |
Job title at time of incident: |
|
|
|
|
|
|
Part of body affected: (shade all that apply) |
Nature of injury: (most |
This employee works: |
|
|
serious one) |
Regular full time |
|
|
Abrasion, scrapes |
Regular part time |
|
|
Amputation |
Seasonal |
|
|
Broken bone |
Temporary |
|
|
Bruise |
Months with |
|
|
|||
|
Burn (heat) |
||
|
this employer |
||
|
Burn (chemical) |
||
|
|
|
|
|
Concussion (to the head) |
Months doing |
|
|
Crushing Injury |
this job: |
|
|
Cut, laceration, puncture |
|
|
|
|
|
|
|
Hernia |
|
|
|
Illness |
|
|
|
Sprain, strain |
|
|
|
Damage to a body system: |
|
|
|
Other ___________ |
|
|
|
|
|
|
Step 2: Describe the incident
Exact location of the incident:
Exact time:
What part of employee’s workday? Entering or leaving work |
Doing normal work activities |
||
During meal period |
During break |
Working overtime Other___________________ |
|
Names of witnesses (if any):
1
Number of attachments:
Written witness statements:
Photographs:
Maps / drawings:
What personal protective equipment was being used (if any)?
Describe,
|
Description continued on attached sheets: |
|
|
|
|
Step 3: Why did the incident happen? |
|
Unsafe workplace conditions: (Check all that apply) |
Unsafe acts by people: (Check all that apply) |
Inadequate guard |
Operating without permission |
Unguarded hazard |
Operating at unsafe speed |
Safety device is defective |
Servicing equipment that has power to it |
Tool or equipment defective |
Making a safety device inoperative |
Workstation layout is hazardous |
Using defective equipment |
Unsafe lighting |
Using equipment in an unapproved way |
Unsafe ventilation |
Unsafe lifting |
Lack of needed personal protective equipment |
Taking an unsafe position or posture |
Lack of appropriate equipment / tools |
Distraction, teasing, horseplay |
Unsafe clothing |
Failure to wear personal protective equipment |
No training or insufficient training |
Failure to use the available equipment / tools |
Other: _____________________________ |
Other: __________________________________ |
|
|
Why did the unsafe conditions exist?
Why did the unsafe acts occur?
Is there a reward (such as “the job can be done more quickly”, or “the product is less likely to be damaged”) that may
have encouraged the unsafe conditions or acts? Yes No If yes, describe:
Were the unsafe acts or conditions reported prior to the incident? |
Yes |
No |
|
|
|
Have there been similar incidents or near misses prior to this one? |
Yes |
No |
2
Step 4: How can future incidents be prevented?
What changes do you suggest to prevent this incident/near miss from happening again?
|
Stop this activity |
Guard the hazard |
Train the employee(s) |
Train the supervisor(s) |
|
Redesign task steps |
Redesign work station |
Write a new policy/rule |
Enforce existing policy |
Routinely inspect for the hazard Personal Protective Equipment Other: ____________________
What should be (or has been) done to carry out the suggestion(s) checked above?
Description continued on attached sheets:
Step 5: Who completed and reviewed this form? (Please Print)
Written by: |
Title: |
Department: |
Date: |
|
|
Names of investigation team members: |
|
Reviewed by:
Title:
Date:
3
Common PDF Documents
Broker Price Opinion Letter Pdf - The form considers the potential impact of zoning laws on property valuation.
For those seeking to understand the significance of the Employment Verification process, it's crucial to access the necessary documentation. You can find essential details about the Employment Verification form through this important guide on Employment Verification.
Chick Fil a Job Application - Initiative taker with a proactive approach to tasks.