Download Planned Parenthood Proof Form in PDF
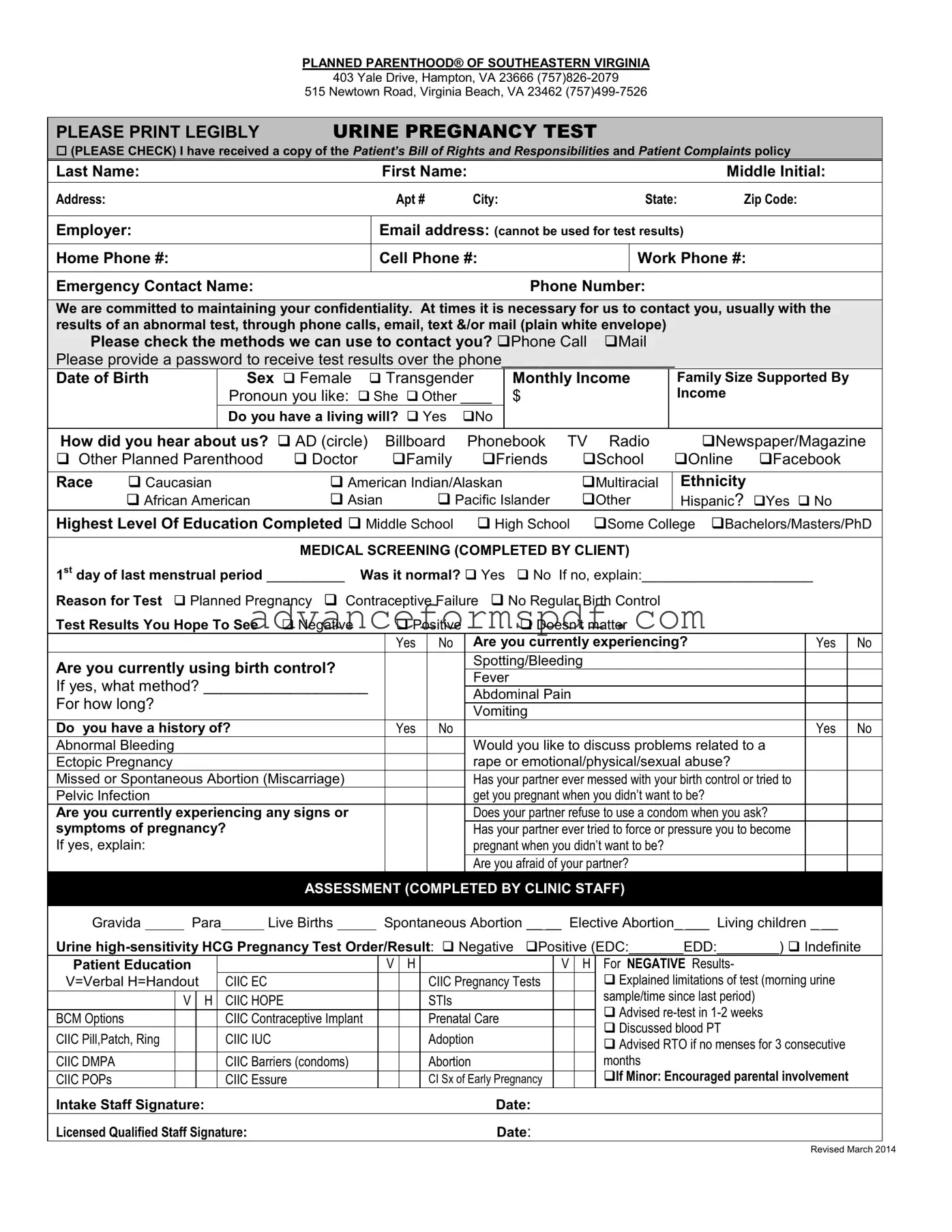
The Planned Parenthood Proof form serves as a crucial document for individuals seeking medical services related to pregnancy testing and reproductive health. This form collects essential personal information, including the patient's name, contact details, and emergency contact information, ensuring that communication remains clear and confidential. It also includes a section for medical screening, where clients can provide details about their menstrual history and any symptoms they may be experiencing. Additionally, the form addresses important aspects such as consent for medical services, acknowledgment of privacy practices, and the option to request language interpretation services if needed. By capturing a variety of data—from income and education level to the reason for the test—the Planned Parenthood Proof form not only facilitates the healthcare process but also empowers individuals to make informed decisions about their reproductive health. The comprehensive nature of this form reflects a commitment to patient care, confidentiality, and informed consent, which are foundational principles in healthcare settings.
Document Data
| Fact Name | Description |
|---|---|
| Provider Information | The form is from Planned Parenthood of Southeastern Virginia, with locations in Hampton and Virginia Beach. |
| Contact Numbers | Two phone numbers are provided: (757) 826-2079 for Hampton and (757) 499-7526 for Virginia Beach. |
| Patient's Bill of Rights | Patients must acknowledge receipt of the Patient’s Bill of Rights and Responsibilities. |
| Confidentiality Commitment | Planned Parenthood emphasizes maintaining patient confidentiality, especially regarding test results. |
| Contact Methods | Patients can choose how they prefer to be contacted, including phone or mail. |
| Medical Screening | The form includes a section for medical screening, where patients report symptoms and medical history. |
| Emergency Contact | Patients are required to provide an emergency contact name and phone number. |
| Consent for Services | Patients must consent to the use and disclosure of their health information as outlined in privacy practices. |
| Legal Requirements | In Virginia, reporting positive test results for certain sexually transmitted infections is mandated by law. |
How to Write Planned Parenthood Proof
Completing the Planned Parenthood Proof form is an important step in accessing medical services. The form collects essential information needed for your visit. After filling it out, you will submit it to the clinic staff, who will review it to ensure all necessary details are provided.
- Print the form clearly and legibly.
- Check the box for the type of test you are requesting, specifically the Urine Pregnancy Test.
- Indicate that you have received a copy of the Patient’s Bill of Rights and Responsibilities and Patient Complaints policy by checking the appropriate box.
- Fill in your personal details: Last Name, First Name, Middle Initial, Address, Apt #, City, State, and Zip Code.
- Provide your Employer, Email address (note that this cannot be used for test results), and phone numbers (Home, Cell, and Work).
- List an Emergency Contact Name and Phone Number.
- Select your preferred methods of contact for test results by checking the appropriate boxes (Phone Call, Mail).
- Choose a password for receiving test results over the phone and write it in the designated space.
- Fill in your Date of Birth and select your Sex (Female or Transgender).
- Provide your Monthly Income and Family Size.
- Choose a preferred Pronoun (e.g., She, Other).
- Indicate whether you have a living will by checking Yes or No.
- Describe how you heard about Planned Parenthood by checking the relevant box.
- Select your Race and Ethnicity by checking the appropriate boxes.
- Indicate your Highest Level of Education Completed by checking the relevant box.
- Complete the Medical Screening section with the date of your last menstrual period and answer questions regarding your health and current symptoms.
- Provide details about any history of pregnancy-related issues or birth control concerns as prompted.
- Sign and date the form at the bottom to acknowledge receipt of the Notice of Health Information Privacy Practices.
- If applicable, have a witness sign the form to confirm that you received the necessary information.
Planned Parenthood Proof Example
PLANNED PARENTHOOD® OF SOUTHEASTERN VIRGINIA
403 Yale Drive, Hampton, VA 23666
515 Newtown Road, Virginia Beach, VA 23462
|
PLEASE PRINT LEGIBLY |
URINE PREGNANCY TEST |
|
|
|
|
|
||||||||
|
(PLEASE CHECK) I have received a copy of the Patient’s Bill of Rights and Responsibilities and Patient Complaints policy |
||||||||||||||
|
Last Name: |
|
|
|
First Name: |
|
|
|
|
|
Middle Initial: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
Apt # |
City: |
|
|
|
State: |
Zip Code: |
|||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Employer: |
|
|
|
Email address: (cannot be used for test results) |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Home Phone #: |
|
|
|
Cell Phone #: |
|
|
|
Work Phone #: |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Emergency Contact Name: |
|
|
|
|
|
Phone Number: |
|
|
|
|||||
|
|
|
|
|
|
||||||||||
|
We are committed to maintaining your confidentiality. At times it is necessary for us to contact you, usually with the |
||||||||||||||
|
results of an abnormal test, through phone calls, email, text &/or mail (plain white envelope) |
|
|
|
|||||||||||
|
Please check the methods we can use to contact you? Phone Call |
|
|
|
|||||||||||
|
Please provide a password to receive test results over the phone____________________ |
|
|||||||||||||
|
Date of Birth |
Sex Female |
Transgender |
Monthly Income |
|
Family Size Supported By |
|||||||||
|
|
|
Pronoun you like: She Other ____ |
$ |
|
|
|
|
Income |
|
|||||
|
|
|
Do you have a living will? |
Yes |
No |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
How did you hear about us? AD (circle) |
|
Billboard |
Phonebook |
TV |
Radio |
|
Newspaper/Magazine |
|||||||
|
Other Planned Parenthood |
Doctor |
|
Family |
Friends |
School |
|
Online |
|||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Race |
Caucasian |
|
American Indian/Alaskan |
|
Multiracial |
|
Ethnicity |
|||||||
|
|
African American |
Asian |
Pacific Islander |
Other |
|
Hispanic? Yes No |
||||||||
|
Highest Level Of Education Completed Middle School |
High School Some College |
Bachelors/Masters/PhD |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL SCREENING (COMPLETED BY CLIENT) |
|
|
|
||||||
|
1st day of last menstrual period __________ |
Was it normal? Yes No If no, explain:______________________ |
|
||||||||||||
|
Reason for Test |
Planned Pregnancy Contraceptive Failure No Regular Birth Control |
|
|
|
||||||||||
|
Test Results You Hope To See |
Negative |
|
|
Positive |
Doesn’t matter |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
Yes |
No |
Are you currently experiencing? |
|
Yes |
No |
|
Are you currently using birth control? |
|
|
|
|
Spotting/Bleeding |
|
|
|
||||||
|
|
|
|
|
Fever |
|
|
|
|||||||
|
If yes, what method? ___________________ |
|
|
|
|
|
|||||||||
|
|
|
Abdominal Pain |
|
|
|
|||||||||
|
For how long? |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Vomiting |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you have a history of? |
|
|
|
|
Yes |
No |
|
|
Yes |
No |
||||
|
Abnormal Bleeding |
|
|
|
|
|
|
Would you like to discuss problems related to a |
|
|
|||||
|
Ectopic Pregnancy |
|
|
|
|
|
|
|
|
|
rape or emotional/physical/sexual abuse? |
|
|
||
|
Missed or Spontaneous Abortion (Miscarriage) |
|
|
|
|
Has your partner ever messed with your birth control or tried to |
|
|
|||||||
|
Pelvic Infection |
|
|
|
|
|
|
|
|
|
get you pregnant when you didn’t want to be? |
|
|
|
|
|
Are you currently experiencing any signs or |
|
|
|
|
Does your partner refuse to use a condom when you ask? |
|
|
|||||||
|
symptoms of pregnancy? |
|
|
|
|
|
|
Has your partner ever tried to force or pressure you to become |
|
|
|||||
|
If yes, explain: |
|
|
|
|
|
|
|
|
|
pregnant when you didn’t want to be? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Are you afraid of your partner? |
|
|
|
|
|
|
|
|
|
ASSESSMENT (COMPLETED BY CLINIC STAFF) |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Gravida |
|
|
Para |
|
Live Births |
|
|
Spontaneous Abortion __ __ Elective Abortion_ ___ Living children _ __ |
|
|||||
Urine
Patient Education |
|
V |
H |
|
V |
H |
For NEGATIVE Results- |
||
V=Verbal H=Handout |
CIIC EC |
|
|
CIIC Pregnancy Tests |
|
|
Explained limitations of test (morning urine |
||
|
V |
H |
CIIC HOPE |
|
|
STIs |
|
|
sample/time since last period) |
|
|
|
|
|
Advised |
||||
BCM Options |
|
|
CIIC Contraceptive Implant |
|
|
Prenatal Care |
|
|
|
|
|
|
|
|
|
Discussed blood PT |
|||
CIIC Pill,Patch, Ring |
|
|
CIIC IUC |
|
|
Adoption |
|
|
|
|
|
|
|
|
|
Advised RTO if no menses for 3 consecutive |
|||
CIIC DMPA |
|
|
CIIC Barriers (condoms) |
|
|
Abortion |
|
|
months |
CIIC POPs |
|
|
CIIC Essure |
|
|
CI Sx of Early Pregnancy |
|
|
If Minor: Encouraged parental involvement |
Intake Staff Signature: |
|
|
|
Date: |
|
|
|
||
Licensed Qualified Staff Signature: |
|
|
Date: |
|
|
|
|||
Revised March 2014
Request for Medical Services and Acknowledgement of Receipt of Notice of Health Information Privacy Practices
PLANNED PARENTHOOD® OF SOUTHEASTERN VIRGINIA
403 Yale Drive, Hampton, VA 23666
515 Newtown Road, Virginia Beach, VA 23462
REQUEST FOR MEDICAL SERVICES AND ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF HEALTH INFORMATION PRIVACY PRACTICES
DATE _______________________________
PATIENT LABEL
Before you give your consent, be sure you understand the information given below. If you have any questions, we will be happy to talk about them with you. You may ask for a copy of this form.
I understand that I must tell the staff if language interpreter services are necessary to my understanding of the written or spoken information given during my health care visits. I understand that free interpretive services may not be immediately available and Planned Parenthood may need to refer me to another health care facility to provide the services necessary for my care.
I understand that the information I will provide is true, accurate, and complete and that my healthcare choices will depend on that information.
I will be given information about the test(s), treatment(s), procedure(s), and contraceptive method(s) to be provided, including the benefits, risks, possible problems/complications, and alternate choices. I understand that I should ask questions about anything I do not understand. I understand that a clinician is available to answer any questions I may have.
Please note that Planned Parenthood Southeastern Virginia is a teaching institution, and that persons in training, under strict supervision, may be involved in some aspects of your care.
No guarantee has been given to me as to the results that may be obtained from any services I receive. I know that it is my choice whether or not to have services. I know that at any time, I can change my mind about receiving medical services at Planned Parenthood.
I understand that if tests for certain sexually transmitted infections are positive, reporting of positive results to public health agencies is required by law.
I will be given referrals for further diagnosis or treatment if necessary. I understand that if referral is needed, I will assume responsibility for obtaining and paying for this care. I will be told how to get care in case of an emergency.
I understand that confidentiality will be maintained as described in Planned Parenthood Southeastern Virginia Notice of Health Information Privacy Practices. I consent to the use and disclosure of my health information as described in Notice of Health Information Privacy Practices.
I hereby request that a person authorized by Planned Parenthood provide appropriate evaluation, testing, and treatment (including a birth control drug or device, if I request it).
I hereby acknowledge receipt of Planned Parenthood Southeastern Virginia notice of health information privacy practices.
Signature of patient __________________________________________________________ Date _______________
I witness the fact that the patient received the above mentioned information and said she/he read and understood same and had the opportunity to ask questions.
Signature of witness _________________________________________________________ Date _______________
CHECK HERE IF PATIENT'S GUARDIAN OR RELATIVE IS LEGALLY REQUIRED TO SIGN BELOW
Signature of any other person consenting ____________________________________
Relationship to patient ___________________________________________________
Date _______________
I witness the fact that the patient's legal guardian (or person consenting in her behalf) received the above mentioned information and said she read and understood same.
Signature of witness _____________________________________________________
Date _______________
Common PDF Documents
Make Your Own Gift Card - Gift letters help lenders assess the financial situation of the borrower.
When engaging in a motorcycle transaction, it's crucial to have the correct documentation in place, such as the Arizona Motorcycle Bill of Sale. This essential form, which can be found through Arizona PDF Forms, clearly records the sale details and facilitates a smooth transfer of ownership, ensuring both buyers and sellers are protected and informed throughout the process.
Mar Template - This record supports informed decision-making by providing comprehensive medication histories.