Download Work Release Form in PDF
When navigating the complexities of employment and legal obligations, understanding the Work Release form becomes essential for many individuals. This document serves as a bridge between personal circumstances and professional commitments, allowing employees to request permission to be absent from work for specific reasons, such as medical appointments, family emergencies, or other personal matters. By submitting a Work Release form, individuals communicate their needs to employers while ensuring that their responsibilities are managed appropriately. The form typically requires details such as the dates of absence, reasons for the request, and any necessary documentation to support the claim. It is crucial for both employees and employers to recognize the importance of this form in fostering transparent communication and maintaining workplace harmony. Moreover, knowing the procedures for submitting and approving the Work Release form can help streamline the process, ensuring that all parties are on the same page and that employees can return to work without unnecessary complications.
Document Data
| Fact Name | Description |
|---|---|
| Definition | A Work Release form allows individuals to leave a correctional facility for employment purposes. |
| Eligibility | Typically, only non-violent offenders qualify for work release programs. |
| Application Process | Individuals must submit an application and receive approval from the facility's administration. |
| Supervision | Participants are usually monitored during their time away from the facility. |
| Governing Laws | Each state has specific laws regulating work release programs; for example, California's Penal Code § 4024.2 governs these forms. |
| Duration | Work release periods can vary, often ranging from a few hours to full days, depending on the program. |
| Benefits | Successful participation can aid in rehabilitation and reintegration into society. |
How to Write Work Release
After obtaining the Work Release form, it is essential to complete it accurately to ensure proper processing. Follow the steps outlined below to fill out the form correctly.
- Begin by entering your full name in the designated field.
- Provide your current address, including city, state, and zip code.
- Fill in your phone number for contact purposes.
- Write your date of birth in the specified format.
- Indicate your employer’s name and address, ensuring all details are accurate.
- List the specific dates and times you will be working.
- Sign and date the form at the bottom to certify the information is correct.
Once completed, submit the Work Release form to the appropriate authority as instructed. Ensure you keep a copy for your records.
Work Release Example
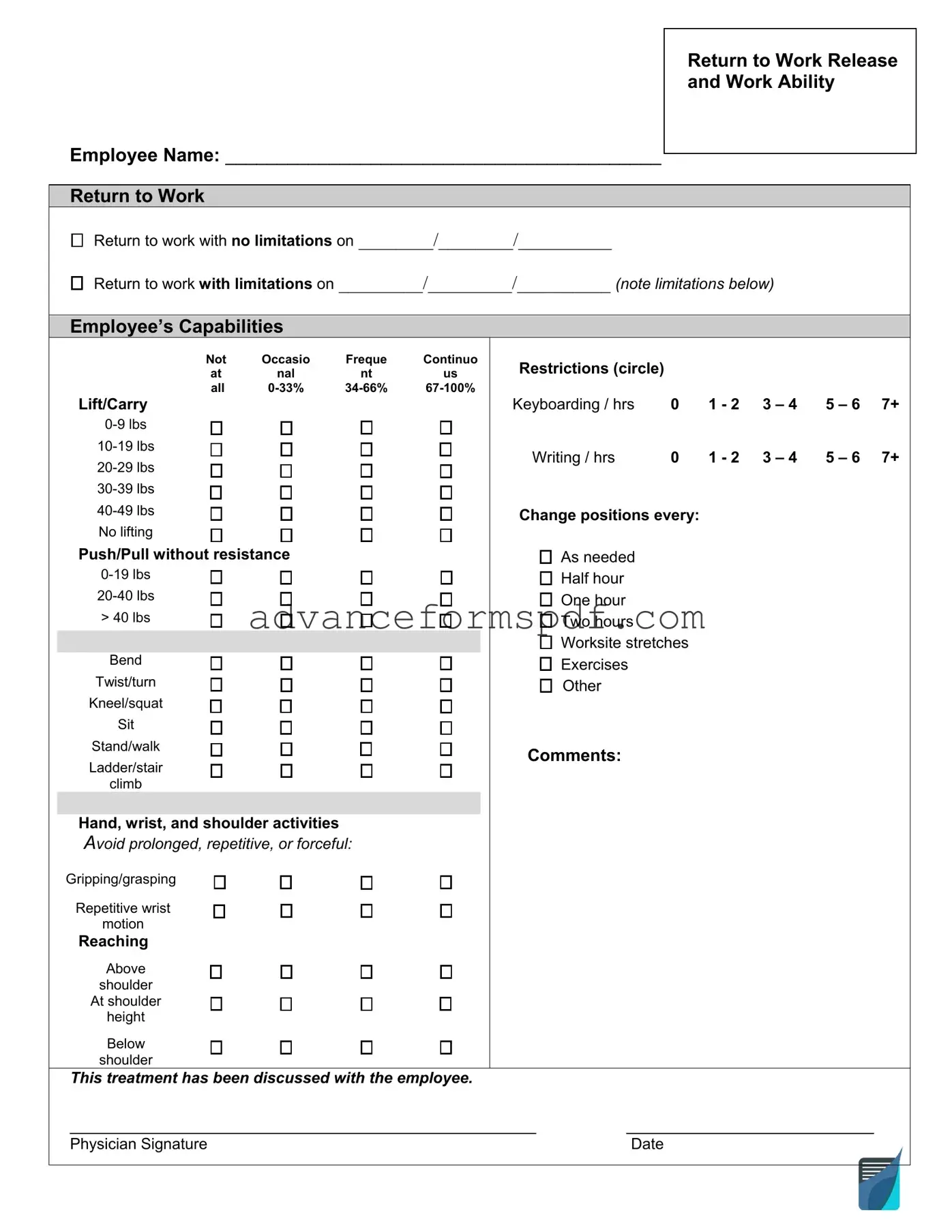
Return to Work Release and Work Ability
Employee Name: __________________________________________
Return to Work
Return to work with no limitations on ________/________/__________
Return to work with limitations on _________/_________/__________ (note limitations below)
Employee’s Capabilities
|
|
Not |
Occasio |
Freque |
Continuo |
|
|
at |
nal |
nt |
us |
|
Lift/Carry |
all |
|||
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No lifting |
|
|
|
|
|
Push/Pull without resistance |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
> 40 lbs |
|
|
|
|
|
|
|
|
|
|
|
Bend |
|
|
|
|
|
Twist/turn |
|
|
|
|
|
Kneel/squat |
|
|
|
|
|
Sit |
|
|
|
|
|
Stand/walk |
|
|
|
|
|
Ladder/stair |
|
|
|
|
|
climb |
|
|
|
|
|
|
|
|
|
|
|
Hand, wrist, and shoulder activities |
|
|
||
|
Avoid prolonged, repetitive, or forceful: |
|
|||
|
Gripping/grasping |
|
|
|
|
|
Repetitive wrist |
|
|
|
|
|
motion |
|
|
|
|
|
Reaching |
|
|
|
|
|
Above |
|
|
|
|
|
shoulder |
|
|
|
|
|
At shoulder |
||||
|
height |
|
|
|
|
|
Below |
|
|
|
|
|
shoulder |
|
|
|
|
This treatment has been discussed with the employee.
Restrictions (circle) |
|
|
|
|
|
Keyboarding / hrs |
0 |
1 - 2 |
3 – 4 |
5 – 6 |
7+ |
Writing / hrs |
0 |
1 - 2 |
3 – 4 |
5 – 6 |
7+ |
Change positions every:
As needed
Half hour
One hour
Two hours
Worksite stretches
Exercises
Other
Comments:
_________________________________________________ |
__________________________ |
Physician Signature |
Date |
Common PDF Documents
Accident Report Form Pdf - Promotes awareness of potential hazards in the work environment.
To facilitate the sale of your recreational vehicle, it's important to use the correct documentation, including the Arizona RV Bill of Sale, which can be found through sources like Arizona PDF Forms. This form not only protects both the buyer and seller but also ensures compliance with the necessary state laws regarding vehicle transfers.
Passport Renewal Application Form - Providing a valid email address on the DS-11 can facilitate communication from the passport agency.
What Is a P45 Form Uk - Employers must provide the P45 to the employee upon termination of their employment.